Is it “ageing” or is it osteoporosis and just happening to practically everyone?
Osteoporosis – what exactly is it?
And why do the joints calcify (develop “rheumatism) as this happens.
And can we prevent this from happening? By Phil Wade
The definition that is closest to the actual description and development of osteoporosis is as follows:
Osteoporosis
os·te·o·po·ro·sis (ŏs′tē-ō-pə-rō′sĭs)
Another that I like is similar:
osteoporosis (ˌɒstɪəʊpɔːˈrəʊsɪs) n
The orthodox view of just how and where the movement of calcium leaves the bone is unclear. Every publication simply refers to the well-known hormone bio-feedback process from pituitary sensing of lowering blood calcium levels to the release of the pituitary hormone PTSH (parathyroid stimulating hormone) to the activation of the parathyroid gland to releast PTH to the resulting stimulation of the osteoclasts to the bone then breaking down and release of calcium into the bone lacunae and from there into the blood vessels and then to …?
And more puzzlingly, some do not even mention low blood calcium as a trigger – just talk about the various – mainly kinase hormones that are involved – and at rather deep, nerdy levels.
Bone loss (osteoporosis) from low intake of calcium
Firstly, low intake of calcium from the diet may cause calcium to move out of bone in order to prop up lowered blood calcium levels.https://www.ncbi.nlm.n ih.gov/books/NBK482128/
ih.gov/books/NBK482128/ 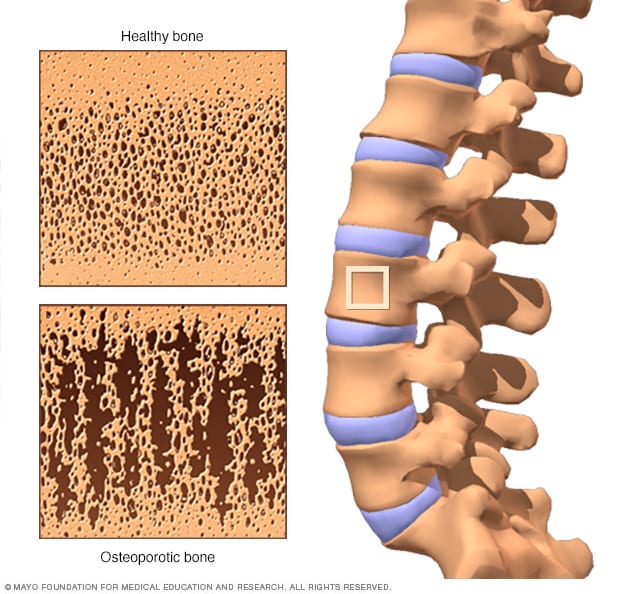 https://www.mayoclinic.org/diseases-conditions/osteoporosis/symptoms-causes/syc-20351968
https://www.mayoclinic.org/diseases-conditions/osteoporosis/symptoms-causes/syc-20351968
Low calcium then is the root cause of most osteoporosis – and not genetic tendency as we have all been told over the decades by our equally ignorant medical fraternity – wrongly, as it happens. And calcium deficiency is therefore the number one reason for osteoporosis, from statistical analysis that the survey Australian Health Survey 2012-14 undertook.
That means that osteoporosis happens slowly, and not so much because of an ageing body as the NIH article implies and that infers that the peak bone mass occurs in the early 20s – rather than from your diet being deficient in calcium over prolonged periods.
Why calcium stores in bone are ever-changing
Firstly, according to the Australian Health Surveys of 2011 and 2015, it is important to understand that not all foods and water supplies contain the calcium they should.
Also that not all calcium in food is absorbed when you eat it.
And I find it interesting that the 2017 Health Survey suddenly stops mentioning imineral deficiency. And that various studies seem to suggest that “bone remodeling” must just keep on happening to our detriment until we are old and riddled with dodgy joints and ever-thinning bones.
Osteoporosis is NOT inevitable.
So, not only is calcium “not absorbed sometimes”, but our food choices also may change from day to day. But more importantly for the purposes of understanding just why it is assumed that osteoporosis is somehow an inevitable course that humans in our society must endure, but in my opinion may prevent, we desperately need to heed the 20-12-14 survey’s apalling findings of gross and widespread deficiency in our diet from the word go – AND do something about it. And is common – shockingly so in my view – in other countries.
That means to you that on many days, your intake of calcium will NOT support bone maintenance, and it will therefore lose nett calcium – which is the difference between what you eat and what you excrete.
And sadly, as you go through the decades of age, inevitably you develop osteoporotic bones. Oh oh – did I mention arthropathy? Please see below.
Constant Calcium Blood Level.
So what specifically triggers the brain response to commence the eviction of calcium out of the bone? Not usually some mysterious, genetic condition but simply low intake of calcium that itself leads to Low blood levels of calcium.
Similarly, after a calcium-rich meal, the subsequently raised blood level causes bone-building.
So, with a perfect daily diet, the bone mass is maintained perfectly over a 24-hour period. (Oops – did I mention a “perfect diet? See below).
How does it do this?
The pituitary gland does this by firstly detecting a low blood level of calcium and in response, releasing a hormone that targets the parathyroid gland and causes it to express parathyroid hormone (PTH). The PTH in turn, directly stimulates the activity of osteoclasts – bone cells that are tasked specifically to break down bone. How about that? Neat, eh?
A calcium-rich diet in turn, causes the reverse process.
So boys and girls – as the USA survey also implies – the only way to really fix the problem in the long term is to constantly supplement with the correct form of calcium.
And I am a bit mortified to finish an article this way but it is most important. And that is to tell you that I have invented what I consider is the prefect supplement.
That is, one that contains ALL the minerals that the bone would obviously store and from which is gains long-term stability.
And that leads me to explain hust how the bone reasserts its mass from periods of low calcium intake. And I write the following lines advisedly, as I have now four clients who attend my clinic whose bone mass and density have both been restored to way greater levels that they had previously. And that this process is a slow one but quite possible.
Pituitary detection and action to restore bones.
Again through pituitary detection – this time the pituitary acts on high blood calcium levels in a good way.
It causes bone-building cells (called osteoblasts) to activate by the release of a thyroid hormone called calcitonin to normalise blood calcium levels. Calcitonin is a little-known hormone that is made in the thyroid gland. Its sole role is to stimulate osteoblast activity to re-build bone, as the diagramme below shows.
It also causes the gut to absorb more calcium via the action of vitamin D3 (cholecalciferol) and also causes the kidneys to retain it.
And I do not know for the life of me why even endocrinologists have argued with me until they are blue in the face that this does not happen.
Prevention – HEY why not try to stop it from happening?
Ao, again I agree with the NIH finding that calcium supplements are an inevitability if your local soil is just not up the the mark.
So I sheepishly but strongly advise you to supplement with a local equivalent of my bone mineral stabilising supplement. We can alter the size of this for adults or children although I am told by my daughter Kirsty – a more recent graduate of advanced nutrition than I – that after the age of 2 YO, required mineral intake of children is much the same as adults, as this survey implies.
And yet the good old Australian Health Survey that claims to be a “second release” of the 2011-13 survey and that also seemingly believes that the W.H.O. values are ideal insists on sticking to those same W.H.O proposed levels which by contrast would leave us all looking rather stunted and sickly by the time we reach adulthood.
I know which one I believe and clearly Kirsty’s lecturers also believe the NIH findings. That’s good enough for me.
By the way – we have invented two different products. The second one covers for all required nutrients (around 105) that the body cannot make for itself and that it needs from the daily diet. So if you or someone you know seems to be developing other possibly preventable chronic ailments, even – especially perhaps – if it is a growing child or teenager, and osteoporosis is common in this age group as you might imagine, then that is why we designed the “Wades Green Smoothi” and “Supasmoothi” – and companion oil blend that completes the deficiency picture.
And the best thing of all? If you are planning a pregnancy then you have the perfect supplement.
One: you will need axtra food anyway.
Two: You will definitely need adequate nutrition to make a healthy, growing child. Clearly the NIH believes that you all have prefect mineral reserves to begin with and maintain throughout a pregnancy. But just in case you haven’t or can’t… remember the Supasmoothi and oil blend.

I have decided to discuss the matter of “Joint calcification and why it occurs” to a follow-up article, as I am sure that you are as exhausted as I am by this stage!
Cheers for now,
Phil Wade
Joint calcification
This movement of calcium back into the blood supply from bone reserves may be – in my opinion – the ultimate cause of why calcium accumulates in cartilage, as the joints may be calcium’s main exit point from bone.
Why? Because also a crystalline formation of calcium in the joints may be created by constant high concentrations of calcium as it emerges into the bloodstream via the joints. The sum total of these events may cause at once a weakening of bone structurealong with micro-bleeds and infection accumulating in the joints probably from occasional micro-bleeds due to the crystalline mass occasionally severing capillaries, with the whole event eventually causing pain. This became “crystal” clear following the brilliantly insightful hypothesis of C W Buckley [Prof. C.W. Buckley, Uni Syd 1928] who said: “All Arthropathy is a Result of Septic Foci”. This hypothesis was based on the findings of the day.
Below right depicts the calcification in the distal joints (phalanges) but also apparently also in the metacarpals and wrist.
:max_bytes(150000):strip_icc()/x-ray-showing-rheumatoid-arthritis-in-hands--colour-enhanced--304788-001-599d9c2a0d327a0011c752c6.jpg)

But reversing osteoporosis, reshaping bones and increasing bone density?
To understand how this condition in the images above and below may be rectified, you need to know how calcium moves in and out of bones and joints.
And then by treating for this aspect, recovery may be possible, no matter what the age. Having said that it is our finding that Herring’s Direction of Cure does influence recovery. That hypothesis says fundamentally that the longer you have suffered from a chronic condition then the longer it takes to heal.
Evidence of reversing the condition
We currently have four MRI results showing “before and after” measurements that highlight beneficial changes according to the respective diagnoses from MDs.
And having said that, we find that the judicious use of TGA-approved Frequency Specific Bioresonance (microcurrent) treatments may help to accelerate recovery from such joint conditions significantly.
Ant according to the Australian Health Survey findings of the extreme rate of calcium and other mineral deficiencies in the average Australian diet, I have creatwd one single supplement that I believe contains every mineral and trace element that will assist this process and that I used in every single case study that showed recovery. See theese hyperlinks regarding the specific and targeted nutritional therapy
Our goal
So creating such nutritional combinations became a goal, and I like to think has helped many such conditions over 40-odd years!

Summing up.
How calcium moves around inside your body.
Under these constantly-changing dietary conditions that regularly see changes in calcium intake, the blood level of calcium is more or less constant while the bone iyself is minutely changing – potentially. Because calcium is necessary also for muscle contraction and normal transmission of nerve impulses that connect the brain to the rest of our body, it is vital that your blood can maintain strict calcium levels at all times. So in times of dietary inadequacy bone breaks down to return stored bone calcium to the bloodstream as mantioned. That’s why the brain monitoring system (pituitary gland) effects this activity, otherwise if the blood calcium level drops too low we would die.
Calcium build-up in joints – how come? – a question for you and me.
So, we were told by our physiology lecturers at Sydney University in 1963 that bone breaks down in the lumen of the bone. From there it is anybody’s guess because certainly nobody discussed the next step as far as I remember, and the only references that I can find are from the Clevelend and Mayo clinics that seem intent on finding mysterious medical conditions rather than simple internal responses to dietary imbalances.
So what do you reckon is happening? To me, it seems that the logical sequence is as follows:
- Widespread osteoporosis occurs in conditions of (well established) dietary deficiencies of calcium.
- The bone breaks down by hprmone bio-feedback to release the stored calcium because blood calcium would otherwise fall to a fatal level – that would cause muscle contraction and nerve stimulation, without which we would die.
- See the end of the article for the The Nerdy bit … Phil’s hypothesis..
The above health survey reveals the shocking information that 94% of Australian schoolgirls between the age of 12 and 16 YO are deficient in calcium.
This would obviously explain the presence of scoliosis, as the statisticians who analysed the survey stated that “calcium deficiency is the number one cause of osteoporosis”.
So, the purpose of this article is to show you how to avoid potential arthropathy that is generally thought to be a genetic ageing process that is unavoidable.
Scoliosis
The survey – that took 4 years to analyse, being released in 2014 following the survey period of 2010 to 2011, goes on to say that nine out of ten girls between 12 YO and 18 YO are likely to be deficient in calcium. And this deficiency by definition is quite obviously a direct cause of scoliosis.
Why? Because the rapid growth spurt at puberty onset quite obviously requires an increase in dietary intake of the elements from which the body is made. All of them! And as calcium and magnesium are the two structural elements required in thje greatest quantity – along with protein – then these requirements must be attend to.
Traditional orthodox medical denial
So why has there been so much denial on the part of the entire medical/dietitian network? It is hard to say, save for the fact that nutritional availability may not form part of their undergraduate curriculum, as it didn’t form part of mine.
That came later, with independent, further studies in the field of Clinical Nutrition. Even then there was a fair bit of denial and ignorance of this matter until the results of the 2011 survey were finally analysed by the Australian Bureau of Statistics and it became shockingly evident.
Lazy medical prognoses over the generations
Might I say that this is a direct and reprehensible flaw in the system of training medical practitioners and pharmacists – and possibly dietitians – at University level over the generations, whose students were all told that osteoporosis and scoliosis were either unknown or genetic. Full stop.
Sadly generations have suffered
So that is what they told parents with young girls, including us.
And this apparent misinformation has led to generations of girls developing this debilitating malady into adulthood, when the bone epiphyses harden and the malformed joint condition becomes irreversible.
And this, in the light of the cause having long been suspected by a a core group of nutritionists from the 90s or even before that, because it flew in the face of the laws of common sense and basic physiology.
So might I now state that, especially given the results of this survey, from now on, please consult a naturopath or nutritionist who is active in this field to establish exactly how to achieve what is a disproportionately higher intake of calcium that is needed for your child. But a word of caution – please ensure that you ask them how to achieve this in balance with other minerals and other nutrient intakes. Because if you add a supplement that is incomplete or imbalanced then it may not have the desired effect – or even a damaging one.
And sadly, the logical conclusion is that in order to stay healthy on an ongoing basis, you will almost definietly have to add at least one complete supplement to your diet.
Arteries too.
It may also accumulate on the outside of artery walls because the arteries are the first vessels to take this exodus.
But all the while, this ongoing deficiency through the years is causing osteoporosis (inadequate bone calcium and structure) according the Australian Health Survey of Usual Nutrient intakes of 2011-12 even though these details are hard to find in the most recent survey.
That is why I believe so few people were privy to this knowledge – and even then only when they self-analysed the results, as nutritionist Henry Osiecki did through those years.
Other calcium problems? Groan!
In pronounced conditions of deficiency may also plunder calcium reserves in artery and heart muscle, as opposed to the artery lumen, so creating potentially coronary chaos.
That’s because you must always have a regulated blood calcium level that is sustained between very narrow parameters by the pituitary gland. This gland constantly monitors blood calcium levels (and other elements) and organises the parathyroid glands, gut and kidneys to “give back” and prevent the excretion of calcium.
Similarly in times of excess, it will order the thyroid gland to store calcium in the bone that is excess to requirements, given sufficient absorption co-factors such as magnesium (see above reference).
These requirements are needed to allow the heart to beat, muscles to contract and many different types of nerves to work.
Known as “electrolytes”, calcium and magnesium work in tandem to allow the contraction and relaxation of these tissues respectively.
And the good part is that consequences of an imbalance in all this may not only be rectified but also prevented by harnessing these natural phenonema!
Maintaining a normal intake of sodium and potassium is also essential, as they are the other two electrolytes that keep our body “ticking”.
Artery calcification – prevention and possible reversal
But it may get worse. As the heart’s arteries are basically en route from this “flow” of concentrated calcium that has just emerged from the bones, calcium may nestle along artery walls.
In that way, calcification may eventually render the arteries brittle by building up calcium plaque, leading into middle age and ultimately cause BP to increase in later life?
I would think that that is the most likely explanation of some otherwise unexplained causes of high BP as we hit the 40s – especially if the cholesterol levels are normal.
Vitamin K2 thought to be made in the liver in small quantities is thought to be responsible for binding calcium in bones and other tissues, so it may protect arteries from undue surface calcification.
Vitamin K occurs in leafy greens and some oils such as flaxseed and walnut oils.
As it is not possible and also unethical to make prescribing suggestions without a consult, please feel free to ring and enquire. But I hasten to add that we may recommend a regime that I use and it has certainly kept my own joints stable, pain free and with minimal swelling (my D.O.B. is January 1944). Of course, the regime naturally includes a combination of choices of a balanced
and complete adjusting of your dietary essential nutrients and/or mineral deficiencies but importantly also offering a way to optimise your health while watching your weight while providing the essentials, aimed at ultimately supporting the body’s ability to remove calcification by biological chelation.
The nerdy bit – how does this work? Phil’s hypothesis.
- And given the above, known, internal sequence of events, and the known ability of joint-cartilage cells to hold calcium, the first thing that happens is that calcium emerges from osteoclast cells into capillaries within the bone crystalline matrix (calcium/protein structures).
- From there the blood in the capillaries containing the calcium flows into the joints, which explains the formation of “false bone” in joints as osteoporosis progresses.
- We were also told that this sequence of events happened when the pituitary released trophic (activating) hormones that targeted the thyroid gland to release a hormone that affected osteoblast (bone-building) cells. Again this is a logical outcome as the pituitary gland is considered to be the master gland in the brain (the Ayveduc “third eye”) that senses the presence of many different elements in the circulation that are essential to life.
- The hormones involved are calcitonin and parathyroid hormone.
- So, in summary, the calcitonin is then released by the thyroid gland under the direction of again, the pituitary (brain) gland and stimulates osteoblast (bone building) cells into action.
- The PTH is also secreted apparently by the tyyroid gland to also act on osteoblasts, but in this case to then itself release PTH to do its thing.